No Pain, Big Gains
Microneedles may mean more flu vaccinations--and less flu

Stephen Nowland
In a phase I clinical trial, Emory researchers have demonstrated the effectiveness and safety of a microneedle patch that could change the way flu vaccines are administered to patients and increase the number of people who opt to get the vaccine.
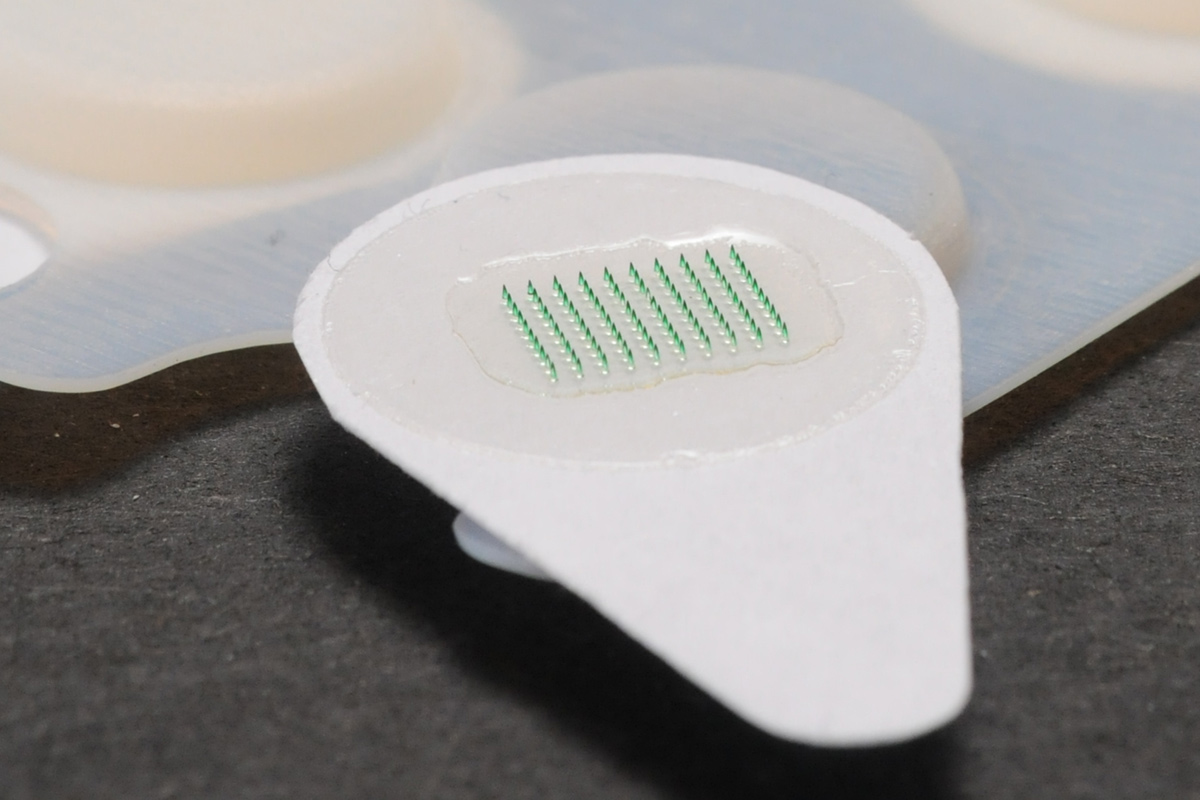
The dime-size patches consist of an array of one hundred tapered microneedles thinner than a human hair at the tip, 350 microns in diameter at the base and 650 microns in length. “They are so small, they’re difficult to see,” says Nadine Rouphael, associate professor of medicine at Emory and principal investigator for the study.
The dissolvable microneedles are filled with the same amount of flu vaccine found in the regular flu shot. When pressed into the skin, the microneedles dissolve in a few minutes, releasing the vaccine and generating the desired anti-body response.
The patch is mounted on an adhesive strip for ease of handling and application, and is removed and discarded after use.
“You can do it yourself because it’s as easy as putting on a Band-Aid,” says Rouphael.
For children and adults who dread needle-and-syringe injections, the patch could be a convenient and pain-free alternative, she observes.
The clinical trial was conducted at the Hope Clinic of the Emory Vaccine Center, led by Mark Mulligan and supported by the National Institute of Biomedical Imaging and Bioengineering of the National Institutes of Health. It was a collaboration between Emory and a team of Georgia Tech researchers led by Mark Prausnitz, Regents professor and J. Erskine Love chair in chemical and biomolecular engineering, who invented the microneedle patch.
The Georgia Tech group worked with Emory researchers led by Richard Compans to fine-tune the patch’s efficacy in mouse models in anticipation of a phase I trial in humans.
For the trial, a flu shot or microneedle patch was administered to one hundred adult volunteers ages eighteen to forty-nine divided into four random groups. In one group, the patch was applied by a health care provider while participants in another group applied the patch to themselves under a nurse’s supervision. The third group received vaccinations via injection by a health care provider, and the fourth group was administered a placebo patch by a health care provider.
The researchers found that flu vaccinations delivered by the patch were safe and effective with no serious adverse effects. Local skin reactions to the patches were primarily faint redness and mild itching that lasted two to three days. Blood sample analysis revealed that the antibody response was similar in those who used the patch compared to those who received a needle-and-syringe injection, and their respective immune responses were still present after six months.
Members of the group who self-administered the patch experienced no problems in terms of safety, how to apply it, or the amount of vaccine they received, indicating the patches had been applied correctly, according to Rouphael.
“It worked as well as if the nurse had applied it,” she says. “When we asked participants in this trial how they felt about it, 70 percent said they preferred the patch over the syringe.”
An examination of used patches showed that the needles had dissolved completely, meaning that patches could be discarded as regular waste, unlike the special handling required of used hypodermic needles.
Flu vaccine patches remain stable at room temperature and have a shelf life of more than a year, she notes. They are easily packaged for transportation and can even be delivered by mail. And since they can be self-administered, the use of patches could eliminate visits to a doctor or health clinic.
Perhaps most important, flu vaccines save lives, Rouphael emphasizes, “and without facing the anxiety and discomfort of an injection, the patch may encourage more people to get annual flu vaccinations.”
In the US, flu season typically begins in October and November and peaks between December and March, sometimes lasting as late as May.
According to the Centers for Disease Control and Prevention (CDC), the influenza virus kills between 3,300 and 49,000 people a year in the US. An exact number cannot be determined because flu-related deaths in adults are not compiled separately. Yet only about 42 percent of adults received a fl u shot during the 2015–2016 fl u season, the CDC reports.
Records are more precise for children under seventeen, 101 of whom died from influenza infections during 2015–2016, when 60 percent of all children received a flu shot, the CDC report stated.
Although complete information on pediatric mortality during last year’s flu season is not yet available, the CDC notes that in years past, between 80 percent and 85 percent of flu-related child deaths occurred in children who had not received a flu vaccine.
Rouphael and her research team hopes their next step is a phase II trial involving a greater number of participants representing a wider age range to include young children and elderly, two groups particularly at risk for contracting the influenza virus, Rouphael explains.
Given the amount of time required to conduct a clinical trial, it’s difficult to estimate when a microneedle fl u-vaccine patch might become available to the public, she says, “but if everything goes well, it could be on the market five years from now per the manufacturer.”
In the meantime, Emory Associate Professor of Pediatrics Evan Anderson is heading the collaboration with Georgia Tech; Micron Biomedical, a startup founded by Prausnitz to license microneedle technology; the Gates Foundation; and the CDC to study the patch as a vehicle for delivering vaccines for measles, mumps, and polio by testing a placebo patch in young children.
“This has been a true team effort and a perfect example of a successful collaboration between Emory and Georgia Tech,” Rouphael says. “The credit goes to the dedicated participants in the study and the wonderful Hope Clinic staff, particularly the lead coordinators, Michele Paine and Regina Mosley.”


